Overview
The peritoneal dialysis (PD) core interventions are practice recommendations designed to prevent infections associated with PD, including peritonitis, exit-site infections, and tunnel infections. These interventions serve as a framework for dialysis facilities caring for people undergoing PD. The interventions are grounded in current evidence and international clinical practice guidelines, with input from a diverse group of stakeholders.
The PD core interventions are available as a manuscript published in the Clinical Journal of the American Society of Nephrology (CJASN), and on this ASN webpage dedicated to supporting the PD core interventions with FAQs and resources. View the free full text version of the article at the button, below.
Watch the Journal Club Webinar Recording June 2026

In this session, faculty discuss the intervention “Standardized Patient and Care Partner/Caregiver Training and Assessment of Competency,” highlighting how to effectively train patients and caregivers, assess their skills, and ensure consistent, high-quality care.
Listen to the Core Interventions for PD Infection Prevention Podcast
Guest Dr. Jeffrey Perl joins host Dr. Tushar Chopra to explore strategies to prevent peritoneal dialysis infections, address gaps in practice, review infection trends, and discuss opportunities for progress through collaboration and team-based care.
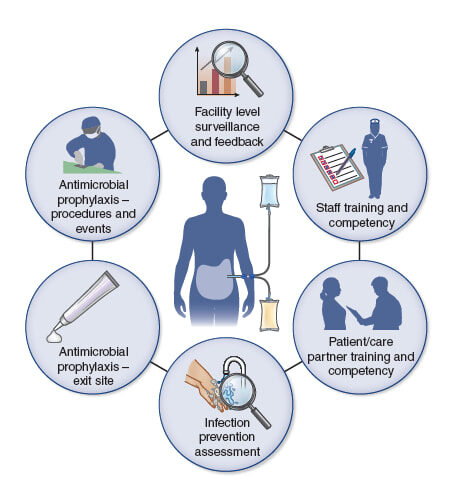
Core Interventions for the Prevention of PD-Related Infections
Facility-level surveillance and feedback.
Identify, monitor, and report on peritonitis, exit site, and tunnel infection events at least quarterly. Use standardized reporting definitions and begin infection reporting from the time of PD access placement. Share results and discuss with the clinical team, including frontline clinical staff. Calculate facility rates and use these rates to benchmark and track rates over time. Optimally, facilities would participate in a national surveillance system that would be developed with stakeholder input.
Rationale
Standardized peritoneal dialysis-related infection rate and outcome reporting across PD facilities has been demonstrated to be feasible in a recent pilot quality improvement project.12 Expanding upon this to a national surveillance system is important for several reasons: 1) to ensure that all facilities are reporting on PD infections using the same definitions and in a similar fashion; 2) to allow for assessment of performance and continuous quality improvement activities; 3) to benchmark infection rates and track rates over time; 4) to allow for apparent cause analyses of all PD-related infections; 5) to identify changes in the microbiology, resistance patterns, incidence, and outcomes of PD-related infections, which may allow for antimicrobial stewardship, outbreak identification, investigation, and containment.4,12,18 Specific challenges which will need to be addressed include: consideration of the reporting of PD infections in small clinics (almost 50% of patients receive care in a clinic with a PD census of less than 26 patients) will be needed where peritonitis rates may fluctuate substantially— particularly if ascertained in too short a period of time.19 Moreover, ISPD benchmarks for peritonitis (target <0.4 episodes per patient year) may not be appropriate in the U.S. where peritonitis rates have been reported to be lower, and a more appropriate lower national benchmark may be needed.9
Frequently Asked Questions
What are the criteria for diagnosis of peritonitis?
For children, diagnosis of PD related infection is described in guideline 8 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, diagnosis of PD related infection is described in the “Definition and measurement of peritonitis” section of the ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment.
What is the definition of an exit site infection?
For children, exit site infections are described in guideline 19.4 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, exit site infections are described in the “Definitions” section of the ISPD Catheter-related Infection Recommendations: 2023 Update.
What is the definition of a tunnel infection?
For children, tunnel infections are described in guideline 19.5 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, tunnel infections are described in the “Definitions” section of the ISPD Catheter-related Infection Recommendations: 2023 Update.
How are peritonitis rates measured and at what frequency?
For children, monitoring of infection rates are described in guideline 22 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, measurement, monitoring and reporting of peritonitis are outlined in the ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment, on table 2 and below.
What are the types/outcomes of peritonitis?
For children, the types of peritonitis are listed in table 5 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, the outcomes of peritonitis are listed in ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment, Table 1.
What are the components of continuous quality improvement (CQI) and how do you conduct an apparent cause analysis (ACA)?
For children, CQI including performance of an ACA is described in guidelines 22.1-22.5 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, CQI including root cause analysis after peritonitis is described under “Prevention of Peritonitis” in the ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment.
Are there examples that demonstrate the use of continuous quality improvement (CQI) to reduce peritonitis rates?
Standardized staff training and assessment of competency.
Provide training that is standardized and includes competency assessment (e.g., knowledge-based testing and direct observation of clinical skills) for all clinical staff, upon hire, and at least annually, and when products/procedures change. Consider individual learning needs in training. Provide preceptorship, timely feedback, and re-training of staff as needed.
Rationale
Initial and ongoing care team education and skills assessments by trained and competent personnel are necessary to drive clinical outcomes and excellence, including the prevention of infections. Infection prevention competency is the proven ability of staff to apply essential knowledge, skills, and clinical abilities to prevent the transmission of pathogens during the education and care of patients on PD. Staff competency impacts patient and care partner/giver education delivery, procedural understanding, and execution of PD clinical skills. Consider various learning styles in any standardized approach to education.20,21
Frequently Asked Questions
Is there a syllabus for teaching peritoneal dialysis to patients and caregivers?
The ISPD published A Syllabus for Teaching Peritoneal Dialysis to Patients and Caregivers and also published a 2025 update, Teaching peritoneal dialysis: A position paper for the International Society for Peritoneal Dialysis.
This ISPD video discusses the training program, both planning and teaching the lesson.
Most of the educational materials available for the training of PD nurses have been developed by industry, including dialysis organizations. Industry clinical educators can provide training syllabi and resources for trainers.
The TEACH-PD Trial, which aims to determine whether a standardized PD training curriculum for PD nurse trainers and adult patients prevents PD-related infections, is ongoing.
How should your organization assess staff competency?
The Centers for Medicare and Medicaid Services (CMS) Conditions for Coverage establish the minimum required standards for staff qualifications and competency. Individual states may impose additional or more stringent requirements. Each dialysis facility must also adhere to its organizational policies, which define processes for monitoring staff competency and ensuring ongoing education and training.
See V584 and V681 on the Centers for Medicare & Medicaid Services. ESRD Surveyor Training Interpretive Guidance: Final Version 1.1 (October 3, 2008).
Standardized patient and care partner/giver training and assessment of competency.
Provide a standardized approach to training patients and care partners/caregivers with consideration of individual learning needs. For example, assessment of learning styles may be standardized using tools such as the Visual, Aural, Read/Write, Kinesthetic Questionnaire in an effort to provide adaptive and individualized training.21 Include a competency assessment (e.g., knowledge-based testing and direct observation of clinical skills). Provide supplemental training at least annually after the initiation of PD and when patient and care partner/caregiver circumstances change, when dialysis products/procedures change, and after certain clinical events (e.g., hospitalization and peritonitis). Provide timely feedback, retraining, and reinforcement to the patient and care partner/ caregiver, as needed. Conduct an initial home assessment, with strong consideration for additional home visits annually and as needed (e.g., for changes to a patient’s health status/home life).
Rationale
Initial and ongoing patient and care partner/caregiver education and competency assessments are necessary to reduce the incidence of PD catheter exit site infection and peritonitis episodes.10,11 Individually optimized training and direct observation of clinical skills are particularly important in reducing and promptly addressing touch contamination events, promoting aseptic procedural techniques, and ensuring ideal PD catheter and exit-site care practices.20,21 Infection prevention competency is the proven ability of patients and care partners/ caregivers to apply essential knowledge, skills, and clinical abilities to prevent the transmission of pathogens during their PD treatments.20-23 Additional research is required to optimize patient and care partner/caregiver training methods, curriculum content, use of telemedicine, and retraining frequency.
Frequently Asked Questions
Is there a syllabus for teaching peritoneal dialysis to patients and caregivers?
The ISPD published A Syllabus for Teaching Peritoneal Dialysis to Patients and Caregivers and also published a 2025 update, Teaching peritoneal dialysis: A position paper for the International Society for Peritoneal Dialysis.
This ISPD video discusses the training program, both planning and teaching the lesson.
Most of the educational materials available for the training of PD patients have been developed by industry, including dialysis organizations. Industry clinical educators can provide training syllabi and resources for trainers.
The TEACH-PD Trial, which aims to determine whether a standardized PD training curriculum for PD nurse trainers and adult patients prevents PD-related infections, is ongoing.
Is there an instrument with which to assess the self-management capacity of patients performing PD?
Individual facilities may have policies that describe how to evaluate whether patients performing PD can manage their care independently.
An article published in 2021 discusses the Development of an instrument to assess self-management capacity of patients receiving peritoneal dialysis: CAPABLE.
How does a facility determine when to reinforce education or retrain?
The Centers for Medicare and Medicaid Services (CMS) Conditions for Coverage establish the minimum required standards for retraining and reinforcement of training. Each organization’s policies define the specific triggers and requirements for these processes within their dialysis facilities. Common triggers include, but are not limited to, episodes of peritonitis, changes in the home environment, care-partner, or dialysis equipment.
See V582 on the Centers for Medicare & Medicaid Services. ESRD Surveyor Training Interpretive Guidance: Final Version 1.1 (October 3, 2008).
Routine patient assessment for infection risk and signs/symptoms of infection.
As part of routine comprehensive patient evaluation, incorporate assessment for signs and symptoms of infection including regular evaluation of the PD catheter exit site and tunnel. Assess patient for infection risk including patient and care partner/caregiver infection prevention procedures. In addition, changes to a patient’s health status, personal circumstances, or home life should prompt an assessment by the care team.
Rationale
Infection prevention practices (e.g., exit-site care, hand hygiene, and the aseptic dialysis procedure) reduce the risk of PD-related infections.18,20,21 When reviewing procedures performed in the home, include an assessment of routine infection prevention practices, including a physical and psychosocial (social, environmental, and cultural) assessment. Examine the PD catheter exit site and tunnel site during the routine monthly visit, with periodic assessment of other aspects of infection prevention including hand hygiene and aseptic technique. During PD access planning, consider infection prevention principles, including optimal exit site location and orientation.24
Frequently Asked Questions
Is there a standardized method for hand hygiene among people performing peritoneal dialysis?
The recommended approach to hand hygiene and method is described in the WHO Guidelines on Hand Hygiene in Health Care. Indications for hand hygiene and hand hygiene techniques begin on page 152, with visual graphics on pages 155 and 156.
Hand hygiene graphics developed can also be found on the WHO website.
What is best practice for PD catheter exit site evaluation at each clinic visit?
For children and adolescents on PD, best practice for PD catheter exit site evaluation is described in guideline 19.2 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, the ISPD Catheter-related Infection Recommendations: 2023 Update includes definitions for exit-site and tunnel infections.
Is there an optimal exit site orientation and location?
For children and adolescents on PD, optimal exit site orientation and location is described in guideline 2.1 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults on PD, optimal exit site orientation and location is described in Creating and Maintaining Optimal Peritoneal Dialysis Access in the Adult Patient: 2019 Update.
What criteria define a peritoneal dialysis exit-site infection, a tunnel infection, or the presence of both?
For children, PD catheter related infections are described in guideline 19.4 and 19.5 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, PD catheter-related infections are described in the “Definitions” section of the ISPD Catheter-related Infection Recommendations: 2023 Update.
Standardized PD catheter exit site antimicrobial prophylaxis.
Apply topical antibiotic cream or ointment to the PD catheter exit site as part of routine exit site care. Perform ongoing surveillance of exit site/ tunnel infection rates, organism type, and resistance patterns, using results to guide the choice of prophylactic agent used in accordance with antimicrobial stewardship principles.
Rationale
PD catheter exit site and/or tunnel infection is an important risk factor for the subsequent development of peritonitis.25 Studies have shown that routine application of either mupirocin or gentamicin to the catheter exit site reduces the incidence of PD catheter exit site infection and peritonitis episodes.26-33 Emerging resistance to mupirocin and gentamicin has been described.29 This is particularly salient where aminoglycoside ointment/cream is the predominant strategy used in most U.S. peritoneal dialysis programs.
Frequently Asked Questions
Does the choice of antimicrobial formulation (i.e., cream, ointment) affect PD catheter stability or associated risks?
According to the ISPD Catheter-related Infection Recommendations: 2023 Update, “Contact between ointments/creams and the PD catheter should be minimized as there have been reports that the polyethylene glycol base in mupirocin can damage polyurethane catheters and that gentamicin cream may damage silicone catheters.”
How should exit-site infections be tracked within the program, and what quality improvement responses are recommended when trends emerge?
For children, monitoring of infection rates and risk factor assessment are described in guideline 22.1 to 22.3 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, refer to the “Monitoring and reporting of catheter-related infections” section of the ISPD Catheter-related Infection Recommendations: 2023 Update.
Where can I find more information about topical antimicrobial agents for use with exit site care?
For children, topical antimicrobial agents for use in exit site care are described in guideline 4.1 and 4.2 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, refer to the “Exit Site Care” section of the ISPD Catheter-related Infection Recommendations: 2023 Update.
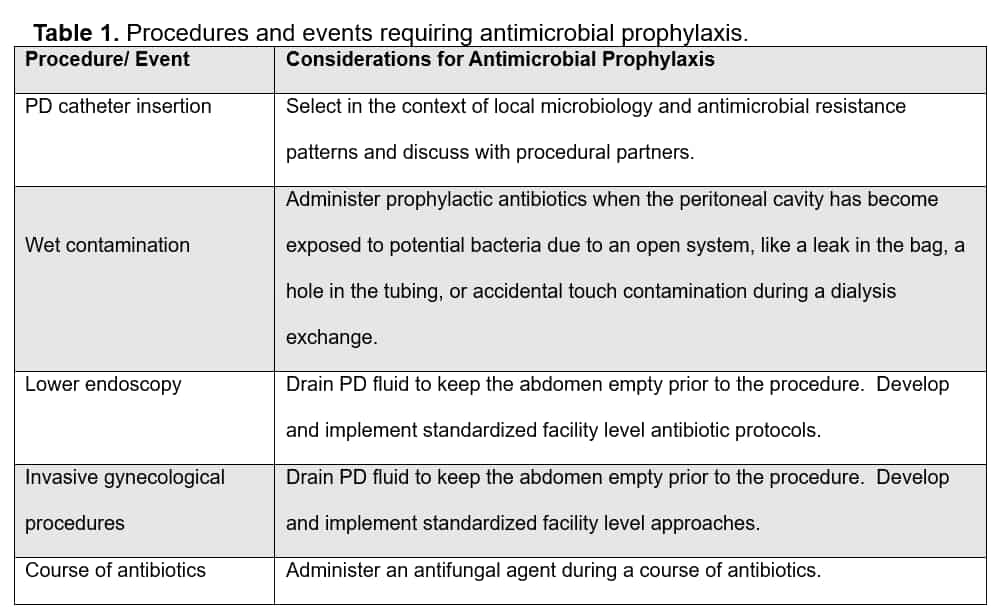
Antimicrobial prophylaxis for procedures/events.
Administer standardized antibiotic prophylaxis to patients prior to undergoing select procedures (Table 1) or on experiencing a wet contamination. Administer antifungal prophylaxis on exposure to antibiotics.34-37
Cover the most likely pathogens associated with procedures and events using prophylactic antimicrobial regimens.18,38 Base the use, choice, and duration of prophylactic antimicrobials on ISPD guidelines, local susceptibility patterns (i.e., antibiogram), individual patient risk, and antimicrobial stewardship principles. Implement processes to promptly identify procedures/events for which prophylactic antimicrobials are indicated, including instructing patients and care partners/ caregivers to inform the dialysis facility when procedures are scheduled or when events have occurred.1,18,38 Communicate with and educate the individual placing the PD catheter, other healthcare facilities, and providers regarding the need for such prophylaxis.
Rationale
The implementation of standardized, program specific protocols may facilitate timely and uniform administration of prophylactic antimicrobials. Guidelines from ISPD recommend prophylactic antibiotics before PD catheter insertion, lower endoscopy, invasive gynecologic procedures, or after a wet contamination episode.1,18,38
Use prophylactic antifungal therapy during antibiotic treatment for any active infection to reduce the risk of subsequent fungal peritonitis.1,34–38
Table 1: Procedures and events requiring antimicrobial prophylaxis
Frequently Asked Questions
What agents should be used for procedures and events requiring antimicrobial prophylaxis?
For children, agents used for procedures and events requiring antimicrobial prophylaxis are described in Guideline 7 and Table 2 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, refer to the “Prevention of Catheter Related Infections” section of the ISPD Catheter-related Infection Recommendations: 2023 Update and the “Prevention of Peritonitis” section of the ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment.
What constitutes a wet contamination and how is it treated?
For children, wet contamination is described in Guideline 7.4 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, refer to the “Contamination of PD System” section of the ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment.
When and how should antifungal prophylaxis be used?
For children, antifungal prophylaxis is described in Guideline 7.1 and Table 2 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, refer to the “Secondary Prevention” section of the ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment.
Should you treat S. aureus carriers prophylactically pre-PD catheter placement?
For children, consideration for treatment of S. aureus carriers is described in Guideline 2.3 (additional considerations) of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, consideration for treatment of S. aureus carriers is described under “Prevention of catheter-related infections” in the ISPD Catheter-related Infection Recommendations: 2023 Update.
What should be considered in preparation for PD Catheter insertion to reduce peritonitis risk?
For children, considerations in preparation for PD catheter insertion is described in Guideline 2 and 3 of the Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update.
For adults, refer to the “Prevention of catheter-related infections” section of the ISPD Catheter-related Infection Recommendations: 2023 Update.
References
- Li PK, Chow KM, Cho Y, et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Perit Dial Int. 2022;42(2):110–153. doi:10.1177/08968608221080586
- Davies SJ, Bryan J, Phillips L, Russell GI. Longitudinal changes in peritoneal kinetics: the effects of peritoneal dialysis and peritonitis. Nephrol Dial Transplant. 1996;11(3):498–506. doi:10.1093/oxfordjournals.ndt.a027318
- Boudville N, Kemp A, Clayton P, et al. Recent peritonitis associates with mortality among patients treated with peritoneal dialysis. J Am Soc Nephrol. 2012;23(8):1398–1405. doi:10.1681/ASN.2011121135
- Al Sahlawi M, Zhao J, McCullough K, et al. Variation in peritoneal dialysis-related peritonitis outcomes in the peritoneal dialysis outcomes and practice patterns study (PDOPPS). Am J Kidney Dis. 2022;79(1):45–55.e1. doi:10.1053/j.ajkd.2021.03.022
- Sethna CB, Bryant K, Munshi R, et al. Risk factors for and outcomes of catheter-associated peritonitis in children: the SCOPE collaborative. Clin J Am Soc Nephrol. 2016;11(9):1590–1596. doi:10.2215/CJN.02540316
- Lambie M, Zhao J, McCullough K, et al. Variation in peritoneal dialysis time on therapy by country: results from the peritoneal dialysis outcomes and practice patterns study. Clin J Am Soc Nephrol. 2022;17(6):861–871. doi:10.2215/CJN.16341221
- Borzych-Duzalka D, Aki TF, Azocar M, et al. Peritoneal dialysis access revision in children: causes, interventions, and outcomes. Clin J Am Soc Nephrol. 2017;12(1):105–112. doi:10.2215/CJN.05270516
- Patel PR, Yi SH, Booth S, et al. Bloodstream infection rates in outpatient hemodialysis facilities participating in a collaborative prevention effort: a quality improvement report. Am J Kidney Dis. 2013;62(2):322–330. doi:10.1053/j.ajkd.2013.03.011
- Perl J, Fuller DS, Bieber BA, et al. Peritoneal dialysis-related infection rates and outcomes: results from the peritoneal dialysis outcomes and practice patterns study (PDOPPS). Am J Kidney Dis. 2020;76(1):42–53. doi:10.1053/j.ajkd.2019.09.016
- Neu AM, Richardson T, De Souza HG, et al. Continued reduction in peritonitis rates in pediatric dialysis centers: results of the standardizing care to improve outcomes in pediatric end stage renal disease (SCOPE) collaborative. Pediatr Nephrol. 2021;36(8):2383–2391. doi:10.1007/s00467-021-04924-0
- Neu AM, Richardson T, Lawlor J, et al. Implementation of standardized follow-up care significantly reduces peritonitis in children on chronic peritoneal dialysis. Kidney Int. 2016;89(6):1346–1354. doi:10.1016/j.kint.2016.02.015
- Al Sahlawi M, Bieber B, Bansal S, et al. Standardized peritonitis reporting: a quality improvement initiative of the optimizing prevention of peritoneal dialysis-associated peritonitis in the United States (OPPUS) study. Am J Kidney Dis. 2024;83(5):692–694. doi:10.1053/j.ajkd.2023.09.004
- Perl J, Fuller DS, Boudville N, et al. Optimizing peritoneal dialysis-associated peritonitis prevention in the United States: from standardized peritoneal dialysis-associated peritonitis reporting and beyond. Clin J Am Soc Nephrol. 2020;16(1):154–161. doi:10.2215/CJN.11280919
- Centers for Medicare & Medicaid Services. End-Stage Renal Disease Quality Reporting System (EQRS) Data Management Guidelines, 2023. Accessed January 2, 2026. https://mycrownweb.org/wp-content/uploads/2023/09/EQRS-Data-Management-Guidelines_2023_Final_9.12.23_vFINAL508.pdf
- Yi SH, Kallen AJ, Hess S, et al. Sustained infection reduction in outpatient hemodialysis centers participating in a collaborative bloodstream infection prevention effort. Infect Control Hosp Epidemiol. 2016;37(7):863–866. doi:10.1017/ice.2016.22
- Patel PR, Shugart A, Mbaeyi C, et al. Dialysis event surveillance report: National Healthcare Safety network data summary, January 2007 through April 2011. Am J Infect Control. 2016;44(8):944–947. doi:10.1016/j.ajic.2016.02.009
- Mehrotra R. Advancing American kidney health: an introduction. Clin J Am Soc Nephrol. 2019;14(12):1788. doi:10.2215/CJN.11840919
- Chow KM, Li PK, Cho Y, et al. ISPD catheter-related infection recommendations: 2023 update. Perit Dial Int. 2023;43(3):201–219. doi:10.1177/08968608231172740
- Knapp C, Li S, Kou C, et al. Trends in outcomes among patients initiating peritoneal dialysis in the United States, 2009-2018. Am J Kidney Dis. 2025;86(4):487–498. doi:10.1053/j.ajkd.2025.06.007
- Figueiredo AE, Bernardini J, Bowes E, et al. A syllabus for teaching peritoneal dialysis to patients and caregivers. Perit Dial Int. 2016;36(6):592–605. doi:10.3747/pdi.2015.00277
- Chow JS, Brunier G, Figueiredo AE, et al. Teaching peritoneal dialysis: a position paper for the International Society for Peritoneal Dialysis. Perit Dial Int. 2025;45(6):327–343. doi:10.1177/08968608251375512
- Beagley L. Educating patients: understanding barriers, learning styles, and teaching techniques. J Perianesth Nurs. 2011;26(5):331–337. doi:10.1016/j.jopan.2011.06.002
- Bernardini J, Price V, Figueiredo A.; International Society for Peritoneal Dialysis (ISPD) Nursing Liaison Committee. Peritoneal dialysis patient training, 2006. Perit Dial Int. 2006;26(6):625–632. doi:10.1177/089686080602600602
- Crabtree JH, Shrestha BM, Chow KM, et al. Creating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 update. Perit Dial Int. 2019;39(5):414–436. doi:10.3747/pdi.2018.00232
- van Diepen AT, Tomlinson GA, Jassal SV. The association between exit site infection and subsequent peritonitis among peritoneal dialysis patients. Clin J Am Soc Nephrol. 2012;7(8):1266–1271. doi:10.2215/CJN.00980112
- Bernardini J, Bender F, Florio T, et al. Randomized, double-blind trial of antibiotic exit site cream for prevention of exit site infection in peritoneal dialysis patients. J Am Soc Nephrol. 2005;16(2):539–545. doi:10.1681/ASN.2004090773
- Strippoli GF, Tong A, Johnson D, Schena FP, Craig JC. Antimicrobial agents to prevent peritonitis in peritoneal dialysis: a systematic review of randomized controlled trials. Am J Kidney Dis. 2004;44(4):591–603. doi:10.1016/s0272-6386(04)00941-2
- Tsai CC, Yang PS, Liu CL, Wu CJ, Hsu YC, Cheng SP. Comparison of topical mupirocin and gentamicin in the prevention of peritoneal dialysis-related infections: a systematic review and meta-analysis. Am J Surg. 2018;215(1):179–185. doi:10.1016/j.amjsurg.2017.03.005
- Chu KH, Choy WY, Cheung CC, et al. A prospective study of the efficacy of local application of gentamicin versus mupirocin in the prevention of peritoneal dialysis catheter-related infections. Perit Dial Int. 2008;28(5):505–508. doi:10.1177/089686080802800514
- Xu G, Tu W, Xu C. Mupirocin for preventing exit-site infection and peritonitis in patients undergoing peritoneal dialysis. Nephrol Dial Transplant. 2010;25(2):587–592. doi:10.1093/ndt/gfp411
- Mahajan S, Tiwari SC, Kalra V, et al. Effect of local mupirocin application on exit-site infection and peritonitis in an Indian peritoneal dialysis population. Perit Dial Int. 2005;25(5):473–477. doi:10.1177/089686080502500512
- Lim CT, Wong KS, Foo MW. The impact of topical mupirocin on peritoneal dialysis infection in Singapore General Hospital. Nephrol Dial Transplant. 2005;20(10):2202–2206. doi:10.1093/ndt/gfi010
- Bernardini J, Piraino B, Holley J, Johnston JR, Lutes R. A randomized trial of Staphylococcus aureus prophylaxis in peritoneal dialysis patients: mupirocin calcium ointment 2% applied to the exit site versus cyclic oral rifampin. Am J Kidney Dis. 1996;27(5):695–700. doi:10.1016/s0272-6386(96)90105-5
- Záruba K, Peters J, Jungbluth H. Successful prophylaxis for fungal peritonitis in patients on continuous ambulatory peritoneal dialysis: six years’ experience. Am J Kidney Dis. 1991;17(1):43–46. doi:10.1016/s0272-6386(12)80249-6
- Robitaille P, Mérouani A, Clermónt MJ, Hébert E. Successful antifungal prophylaxis in chronic peritoneal dialysis: a pediatric experience. Perit Dial Int. 1995;15(1):77–79. PMID: 7734569
- Wadhwa NK, Suh H, Cabralda T. Antifungal prophylaxis for secondary fungal peritonitis in peritoneal dialysis patients. Adv Perit Dial. 1996;12:189–191
- Lo WK, Chan CY, Cheng SW, Poon JF, Chan DT, Cheng IK. A prospective randomized control study of oral nystatin prophylaxis for Candida peritonitis complicating continuous ambulatory peritoneal dialysis. Am J Kidney Dis. 1996;28(4):549–552. doi:10.1016/s0272-6386(96)90466-7
- Warady BA, Same R, Borzych-Duzalka D, et al. Clinical practice guideline for the prevention and management of peritoneal dialysis associated infections in children: 2024 update. Perit Dial Int. 2024;44(5):303–364. doi:10.1177/08968608241274096
- Chow JS, Adams K, Cho Y, et al. Targeted education ApproaCH to improve peritoneal dialysis outcomes (TEACH-PD): a feasibility study. Perit Dial Int. 2020;40(2):153–163. doi:10.1177/0896860819887283
- Chow JSF, Boudville N, Cho Y, et al. Multi-center, pragmatic, cluster-randomized, controlled trial of standardized peritoneal dialysis (PD) training versus usual care on PD-related infections (the TEACH-PD trial): trial protocol. Trials. 2023;24(1):730. doi:10.1186/s13063-023-07715-0
Page last reviewed on May 5, 2026.
